
28. The Drop

“[The Drop] is the emotional and physical affects of the release and drop of endorphins in the body after an intense experience.”
~ Neil Morbey, as inspired by London Faerie and Brene Brown
In the circles in which I am a part, “the/a drop” is often used to describe the feeling associated with feeling down after something good (or at least intense) has happened. This could be a first date, a fun vacation, a fun party, or whatever. Perhaps a similar affect can occur in survivor’s guilt: a feeling of guilt or sadness that can occur after someone survives a traumatic event that others did not.
In either case, it seems like the emotional hangover should be a positive one: “something great happened, and so I feel good now and will for a while!” or, in the case of survivor’s guilt: “something terrible could have happened (or could continue to be happening) to (or around) me, but it didn’t: I’m so glad!”
However, this is often enough not the case that people have named it.
Common, too, are these feelings after facial feminization surgery (enough that Facial Team, one of Europe’s leading facial feminization surgical teams, put together a compilation of potential emotional outcomes from FFS).
I am in the middle of (slowly coming out of) this fairly common post-FFS drop. As my body starts to come back to life, and as my head starts to recover, I am feeling better and better. However, there are still elements that I find disheartening, and I think it is valuable to mention them here.
But first, I have to explain the FFS procedures I underwent, what the target outcomes were, and where they were successful… and where they weren’t.
Targets
There were five targets for my FFS:
Reduce my Adam’s Apple to a size consistent with androgyny at worst, cis-female at best
Recontour my jawline to represent a less masculine appearance
Reshape my nose to represent a less masculine form
Reshape my eyes and brow to represent a less masculine form
Advance my hairline to create a more upside-down U shape (common in women) as opposed to the M shape (common in men)
Each of those targets had a specific strategy for making the desired changes:
Adam’s Apple
My doctor would use the “fiberscope and needle” method of chondrolaryngoplasty (more commonly known as a “tracheal shave”) to determine the precise and maximum amount of cartilaginous tissue that could be removed from in front of my larynx.
Essentially (don’t quote me, and don’t @ me if you’re a doctor who knows better than I do), the larynx consists of several key and important structures:
The vocal folds, or vocal cords. These come together and vibrate when you want to talk or sing.
The trachea. This is the tube-like pathway above and below the vocal folds that brings air to and from the lungs below
Cartilage. This is present in various places both above and below the vocal folds and creates the more rigid structures of the trachea’s walls.
Other soft tissues. There’s a lot I’m probably missing, but for this story it doesn’t matter: Consult your physician or a dubious online information repository or AI-chatbot for more information.
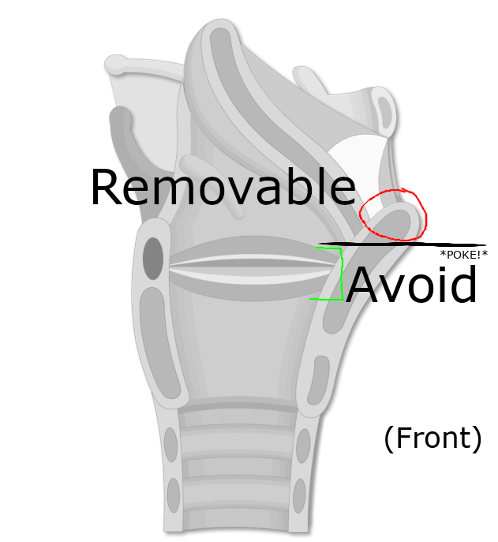
To reduce the visible Adam’s Apple, cartilage is removed from above the vocal folds. A well-skilled, kind, or otherwise tort-averse surgeon will be mindful to not remove cartilage at or below the vocal folds, as the vocal folds rely on the structure provided by that cartilage to function properly. Fortunately, most of the prominent features of an Adams Apple are above the vocal folds in a location known unambiguously as the Laryngeal Prominence.
To identify the location of the vocal folds to facilitate not removing too much cartilage (while still removing as much as possible), some doctors use the “fiberscope and needle” method. This, quite literally, involves sticking a scope down a throat and then stabbing it repeatedly with a small needle to see where the needle-stab location on the outside of the larynx corresponds with the proximity to the vocal folds. Once the safe limits are determined, they are marked and then everyone hopes the patient won’t be too grumpy about playing the role of stuffed-red-tomato while under anesthesia:
A side-view of a trachea facing to the right with a few illustrative markings for convenience:

Jawline
My doctor would perform a sliding genioplasty, body cortectomy, and angled osteotomy to feminize the chin and jawline. Essentially, these (in order) mean:
Cut off the chin, divide it into two slightly smaller pieces, and reattach it recessed slightly. Use some metal and screws to make sure stuff doesn’t slough off later.
Remove the back corners of the jaw
Make any additional cuts or shaves to smooth things out
No big deal.
The below image illustrates (on my actual skull) where these modifications were to occur:

The incisions to access these areas of bone would all be inside my mouth, between my cheeks and my gums. The lower lip would be pulled down to fully expose the chin bone, whereas the rear incisions would just be pulled open. Think of whatever creative metaphor for this that is the most disturbing to you: the mid-surgery photos I have are likely more disturbing.
Nose
This is all art. Essentially, it is more common (although not universal) for men’s noses to be longer and point downward, whereas women’s noses are shorter and point upward. See the following for reference:

The techniques here involve removing and reshaping various cartilage in the nose, and then reinserting it and sewing everything up. All incisions are within the nostrils.
Eyes and Brows
Men typically have more pronounced orbital rims and brow ridges. Simply put, men’s skulls beneath the eyebrows (and the space between the eyebrows — or, if you are like me or Frida Kahlo, the center of the single eyebrow) is more prominently forward (on average) than women’s skulls in the same place.
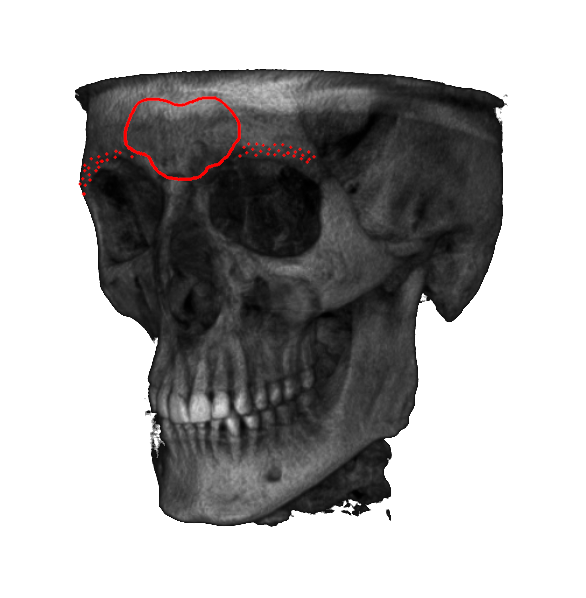
The process to address this is many of the same kinds of techniques described in the Jawline section: chop up and grind down the bone (but with fancy words). In detail, the plan included:
File down the bone above each of the eyes to create a less-prominent brow ridge directly behind each of the eyebrows
Remove a section of bone directly above the nose (between the eyebrows) and re-seat it recessed back slightly. This section of bone can’t be filed down as it is directly in front of a sinus cavity, so filing it down could result in a weak skull (We want strong woman skulls, not flimsy-and-likely squishy head-bones. Megan Rapinoe wouldn’t abide a weak head like that, it’s useful for cases where you need to head-butt things, which, as she demonstrates regularly, is quite feminine and impressive).
{kind=link}
The below image illustrates (on my actual skull) where these modifications were to occur
The incision to access this area would be from ear-to-ear across the top of my head, passing right long the hairline (this incision is also part of the hairline adjustment). The skin will be peeled down Hannibal-style to expose the brow ridge area, and even the top of the nose bone (might as well file that down a bit while we are in there…), and then reattached with as many as 75 staples and a bunch of stiches, as well as a few hopes and dreams (which should have an easier time getting in there, what with the giant forehead-sized opening in the front of my head).
Hairline
Once everything else is sufficiently mangled and/or Dremeled, a section of scalp above the hairline (specifically corresponding to the gaps in the M-shaped hairline would be removed, and the scalp behind it would be freed from my skull via medical spatula, pulled forward, and attached to the incision created during the brow-ridge work. Some sub-dermal ligature (there’s probably a better, more accurate medical term for what is basically “surgical rope”) attached to a few screws (also used to keep the previously-removed sinus-bone in place) would help pull the scalp forward to anchor it in place for reattachment.
Hits
Now that I’ve successfully lost half of the readers to nausea or horror (or both), I can move on to where everything went well:
Jawline — Success, with some notes:
All of the bone work went well, although the swelling of the soft tissue around it is brutalNose — Success, with some notes:
Looks great, although it is quite stiff. I am led to believe that this stiffness may subside with timeBrow — Success, with some notes:
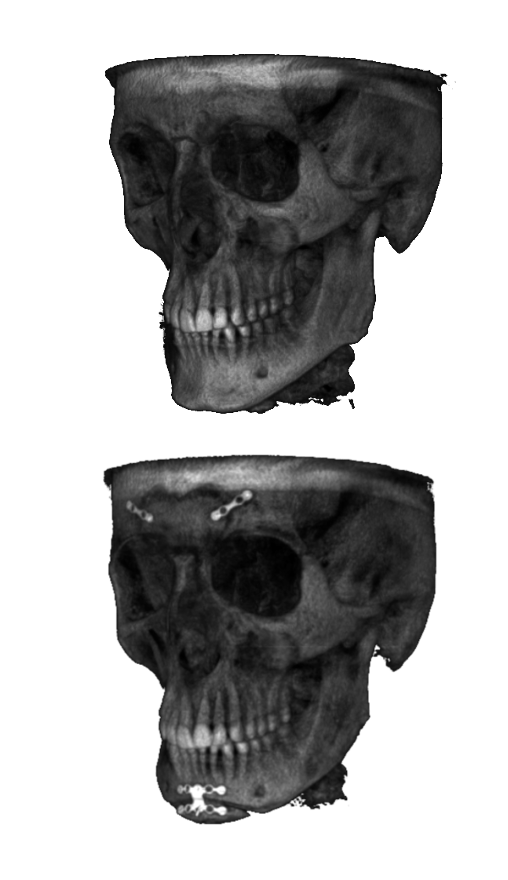
All of the bone work went well, although now there is a leak from my front sinus leading to air bubbles getting trapped between my forehead bone and my forehead skin when I exhale too strongly (blowing my nose or coughing for example). This air should reabsorb, and the leak should seal itself over time.Hairline — Success!
Here’s a before and after of my actual skull, where the described bone work (and metal plates used to reattach things) is clearly visible:
Misses
The most noticeable miss is my Adam’s Apple.
As I previously described, only certain portions of the cartilage can be safely removed (provided “being able to speak” is a talent that we want to retain). The doctor spent twice as much time working on my Adam’s Apple as normal, removing every single bit of tissue that could safely be removed.
The end result is an Adam’s Apple that is still larger than those of most cisgender men.
This is really quite disappointing, as it is a major (in my opinion) indicator of gender, and one that I specifically wanted to have properly addressed (i.e., removed completely). I believe my doctor did as well as any doctor could with cartilage removal. At this point, I am looking into other procedures that may be able to reshape the entire larynx, reducing the size and changing the shape as needed to reduce my larynx to female proportions… although these surgeries (specifically, feminization laryngoplasty) are not commonly performed and can have adverse effects on speaking ability (raspy voice, etc.).
We’ll see what I do moving forward, other than trying to avoid being seen in profile-view.
A less permanent disappointment (although one that does bring me some frustration) is the amount of swelling (and numbness) around my jaw, specifically my chin. I know that this swelling will subside eventually, and I should regain full felling of my chin, lower lip, and lower incisors, but in the meantime I struggle with eating, speaking, and many facial expressions (never mind looking like Joe Swanson’s face from the nose down). Apparently my swelling is less than some people deal with, but it is still frustrating.
{kind=link}
The Future
The swelling and numbness will pass, but, in the interim, I am doing my best getting by with very soft foods and the indefatigable support of those around me. Soon I will be working regularly again, and I will be seeing my child for the first time in weeks in a few days. And, despite the physical setbacks, I am moving forward with indefatigable resolve to update all of my legal documents prior to the new administration’s inauguration.
I believe I am on the right track — not just with my documents, but with my recovery — and will probably start feeling better soon.
Although “Soon,” if the people who have gone through this before me are to be believed, may take the form of months, not weeks.
I think you look great, and I hope the swelling resolves more quickly than you expect.